Bursitis: Trochanteric
Pathophysiology/Etiology
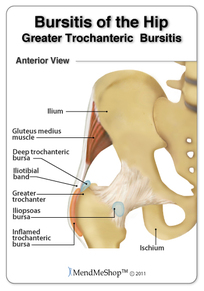
- Common cause of hip pain related to inflammation of one of the three main bursae of the hip: the trochanteric bursa, the iliopsoas bursa, or the ischiogluteal bursa.
- Caused by overuse or degenerative changes in the bursae.
- Frequently seen by sports practitioners.
- Occurs in 5.6 patients per 1000 adults and is often referred to as “greater trochanteric hip pain.”
- Etiology is multifactorial and can affect patients of all ages; however, it occurs most frequently in middle aged to elderly patients. The iliotibial band (ITB) and fascia lata act as a lateral tension band that resist tensile strains on the concave aspect of the femur and is often implicated as source of TB. Gluteus medius tears also referred to as the “rotator cuff tear of the hip” are found in 22% of elderly patients and is a frequent source of lateral hip pain.
Signs/Symptoms
- Characterized by chronic lateral hip or buttock pain exacerbated by active abduction, passive adduction and direct palpation.
- Increased difficulty and pain with activity and pain worse in the evening.
- Pain may radiate down the leg to the level of insertion of the iliotibial tract on the proximal tibia.
- Will have tender great trochanter and positive “jump sign” when the greater trochanter is palpated.
Diagnostic Tools
- Subjective exam: description of lateral hip pain with referral to the insertion of the iliotibial tract on the proximal tibia and possible activity limitations that require use of the hip. Patient will have pain that is worse in the evening.
- Objective exam: palpation of the lateral hip and trochanter area, active movement (hip abduction), passive movement (hip adduction). Manual muscle examination and ROM should be used to help rule out other conditions along with other special tests for the hip (leg-length discrepancy, Scours, FABER, Log-rolling etc.). The patient may have a positive Trandelenburg (especially if the gluteus medius is involved), Jump test, Obers (ITB), or Modified Thomas Test (for TFL). Patient may present with normal hip rotation and movement may reproduce pain (extra articular structure).
- Radiographs are not typically helpful in diagnosing bursitis unless the bursa has calcified. There is a lack of universality in diagnosing lateral hip pain as TB, therefore the hip joint should be screened and all other possibilities ruled out first.
Prognosis
- With conservative interventions used individually or combined, the cure rate is over 90%. However, recurrence is common and patients often undergo multiple nonoperative treatments with temporary or incomplete pain relief.
Treatment
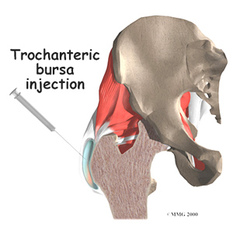
- Conservative treatment including activity modification, physical therapy, weight loss, corticosteroid injection, and NSAIDS.
- Surgical treatments are available for more severe and chronic cases.
- Surgery typically includes release of the ITB and fascia lata. Other surgeries include bursectomy, longitudinal release (Z-plasty) and gluteus medius repair. Improvement in pain symptoms is reported at 88-100% in patients. Risks are significantly higher and include risk of infection and abductor weakness secondary to denervation of the gluteus medius.
- Injection alone showed an 2.8 improvement on the VAS. Baseline activity improvement ranged from 49-100%. Injections are relatively low in complications but may produce, skin irritation, swelling and temporary pain in the area of injection.
- Multimodal approaches that included rest, PT, ultrasound, steroid injections, ice, and heat, 66-83% of patients were able to return to sports and labor intensive occupations after 3 months.
- Home Exercise Programs (HEP) that focus on piriformis and ITB stretching, gluteal strengthening, straight leg raises and assisted squats, 34% of patients were able to return to normal activity, 40.8% had significant improvement (with at least 1 grade of improvement on the VAS).
- Low-Energy Shock Wave Therapy (SWT) shows an average improvement of 3.9 on the VAS in patients. 64-76% of patients reported being able to resume normal physical activity. This intervention has minimal complications, but may include skin irritation or erythema.
Prevention
Differential Diagnosis
- Maintain a healthy weight by diet and exercise.
- Stretching of hip and soft tissues before and after strenuous activity.
Differential Diagnosis
- Based on subjective and objective measures as previously described. Bursitis is often treated by physical therapy. Referral is suggested int he presence of a cluster of red flags.
