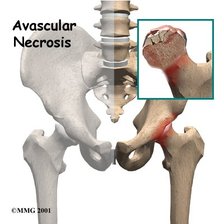
Avascular Necrosis (AVN) of the Femoral Head
Pathophysiology/Etiology
- Definition: progressive ischemia and secondary death of osteocytes and fat cells which cause the bone of the femoral head to alter and collapse, ultimately leading to the development of degenerative athritis
- AKA: osteonecrosis, aseptic necrosis, ischemic bone necrosis
- "Avascular necrosis" is the term used for posttraumatic causes because they originate with ischemia due to interruption of blood flow
- "Idiopathic necrosis" is the term used for an unknown or unestablished etiology of the necrosis
- most common cause is trauma
- glucocorticoid use and alcoholism represent 90% of all non-traumatic causes
- most common in active males
- Age: 30-50
- Conditions Associated with AVN:
Trauma*
Iatrogenic
-use of glucocorticoids*
-alcohol*
Hematological
-sickle cell anemia
-thalassemia
-polycynthemia
-hemophilia
-myeloproliferative disorders
Metabolic
-Gaucher disease
-hypercholesterolemia
-pregnancy
-chronic renal failure
-Hyperparathyroidism
-Cushing’s disease
Autoimmune disease
-systemic lupus erythematosus
-rheumatoid arthritis
Gastrointestinal
-Chronic pancreatitis
Orthopaedics cause
-congenital hip dislocation
Signs/Symptoms
- May be asymptomatic during early stages
- Initial mild hip pain that may last for weeks
- Hip pain that gets progressively worse over time (insidious onset)
- Possible groin or anteromedial thigh pain
- Pain worse on weightbearing, but may be present at rest (intermittent)
- Antalgic gait with a gluteus minimus limp (possible Trendelenberg)
- Limited hip IR/flexion/abduction ROM
- Palpation over hip joint reveals tenderness
- Hip joint stiffness
- Hip dislocation
- Special Test
Diagnostic Tools
- Conventional radiography is the most convenient and inexpensive firsts line of investigation, but is not sensitive in detecting early AVN lesions
- Bone scintigraphy helps catch AVN at an earlier stage, but is not specific for diagnosing AVN by itself
- MRI is more sensitive than plain radiograph for diagnosing early-stage AVN, but is the most expensive option
- Radiologic findings present a flattening followed by collapse of the femoral head
Prognosis
- Affected by the stage of the disease
- Clinically diagnosed AVN is progressive (collapse of the femoral head) in 70-80% of patients who are managed nonoperatively.
Treatment
- Conservative intervention is aimed at reducing stressors through the hip joint and utilizing support, but operative intervention is usually recommended
- Conservative management includes rest and reduction of weight bearing.
- Minimizing or eliminating glucocorticoid use if the underlying condition allows
- Bisphosphonate use in reducing the rate of collapse of the femoral head is controversial
- Surgical therapy includes core decompression, osteotomy, bone grafting and hip arthroplasty
- Platelet-rich plasma (PRP) is a novel nonsurgical treatment for degenerative AVN of the femoral head which uses an autologous source of cellular growth factors (GFs) that aids in tissue repair.
Prevention
- Reduction in alcohol consumption
- Conservative use of corticosteroids and immunosuppressants as much as possible
- Prevention of diabetes mellitus through healthy living with proper diet and exercise
Differential Diagnosis
- If AVN is undiagnosed and is the suspected cause of hip pain, referral to a physician for imaging and possibly to an orthopedic surgeon for discussion of treatment options is necessary.
