Stress Fractures
Pathophysiology/Etiology
-- Causes: changes in running surface, use of inadequately cushioned footwear, or presence of female athlete triad
Signs/Symptoms
Diagnostic Tools
Prognosis
Treatment
Acute Phase
Prevention
Diet
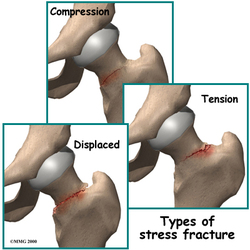
- Microscopic in nature and does not show displacement
- Commonly, initial radiography does not show the fracture
- Most commonly present as exercise-induced groin pain
- Common presentation #1: Young, high level athlete, who participates in repetitive high impact sports (distance running); location is most commonly in the pubic ramus.
-- Causes: changes in running surface, use of inadequately cushioned footwear, or presence of female athlete triad
- Common presentation #2: Older adult with a stress fracture of the femoral head or neck.
Signs/Symptoms
- Pain described as aching or deep aching
- Pain increases with activity and improves with rest
- Compensatory gluteus medius gait
- Pain localizing to a specific area of bone (localized tenderness)
- Positive Faber's test
- Pain reproduced by weight bearing, heel strike, or hopping test
- Pain reproduced by translational/rotational stress (exquisite pain in response to active resistance to hip adduction/hip adduction combined with external rotation)
- Thigh pain reproduced by the fulcrum test (femoral shaft fracture)
- Possible local swelling
- Increased tone of hip adductor muscles; limited hip abduction
- Night pain (femoral neck stress fracture)
Diagnostic Tools
- Patient History
- Faber's test
- Fulcrum Test (high clinical correlation with femoral shaft stress injury)
- Heel strike test
- X-ray’s
- Bone Scans
- MRI
Prognosis
- Varies per patient presentation
- Young patients and those with healthy diets heal faster
- Weight bearing restrictions should be removed within 4-6 weeks
- Patient should be able to ambulate community distances independently without pain within 8-12 weeks.
Treatment
Acute Phase
- Protect the joint (PRICEMEM - protection, rest, ice, compression, elevation, manual therapy, education, modalities)
- Protection and Rest - Crutches should be used for non-weight bearing status and increasing weight bearing over first 4-6 weeks according to pain and presentation.
- Ice – To assist with pain reduction and any inflammation that may be present
- PROM and AAROM may be introduced in this phase with pain free activity.
- Medications and Modalities – may aid in pain modulation
- Therapeutic exercise may be increased with weight bearing and tolerance
- CKC (Closed Kinetic Chain) exercises are recommended to decrease stress on injury site.
Prevention
Diet
- Appropriate calorie intake
- Ample Ca+ and vitamins
- Resistance Training (> or = 2x per week, 6-10 exercise, covering the major muscle groups)
- Aerobic Exercise with appropriate periods or rest.
